

Advanced Surgical Treatments
Dr. Womack's 2-year Minimally Invasive Gynecologic Surgery (MIGS) fellowship gives her advanced experience surgically managing complex gynecologic diseases. She is able to offer major surgeries through small incisions which allow you to go home the same day. Minimally invasive surgeries have lower blood loss, infection rates, and hospital stays compared to open surgeries. Her minimally invasive techniques also focus heavily on adhesion reduction and fertility restoration for those couples struggling with infertility.
Endometriosis Excision
Endometriosis is defined as tissue similar to endometrial glands and stroma (tissue normally on the inner wall of the uterus) that grow outside of the uterus. Common places endometriosis can grow are the pelvic walls, ovaries, behind the cervix, and rectum.
Myomectomy Fibroid Removal
Fibroids, or leiomyomas, are benign tumors of the muscle of the uterus that are stimulated by estrogen. Fibroids are fairly common, but not all of them cause issues that need to be addressed. There is a wide variety of fibroid types characterized by size and location.
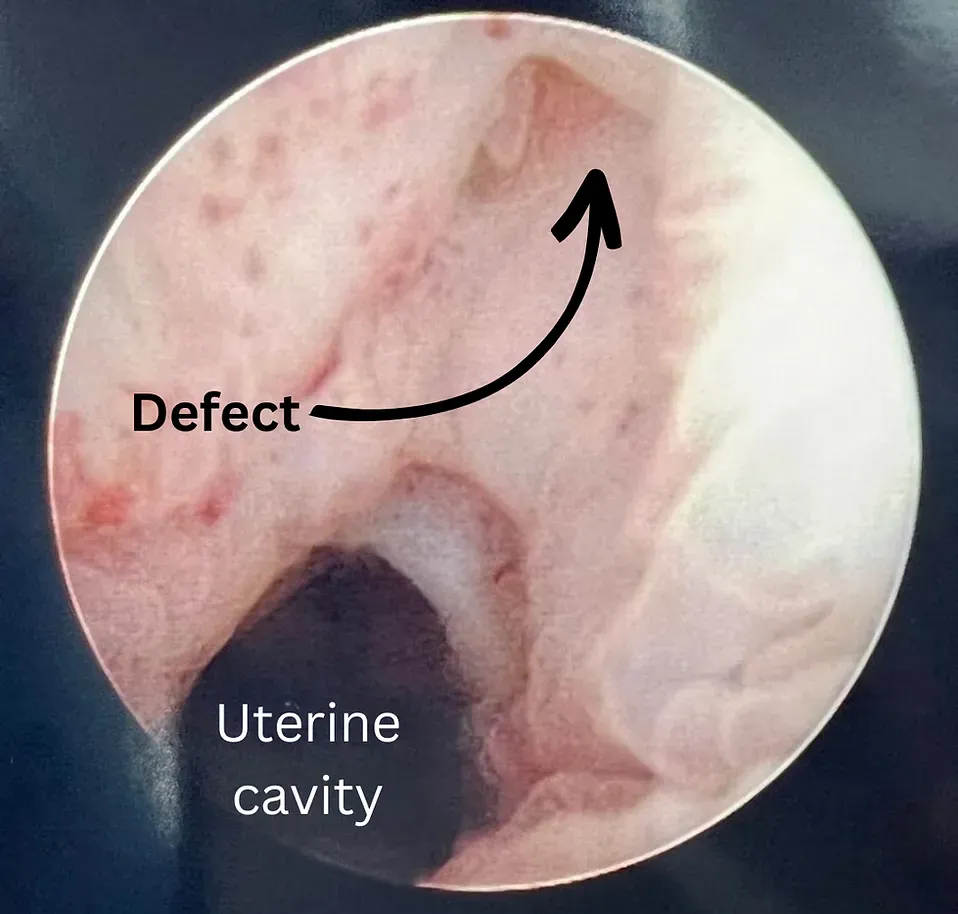
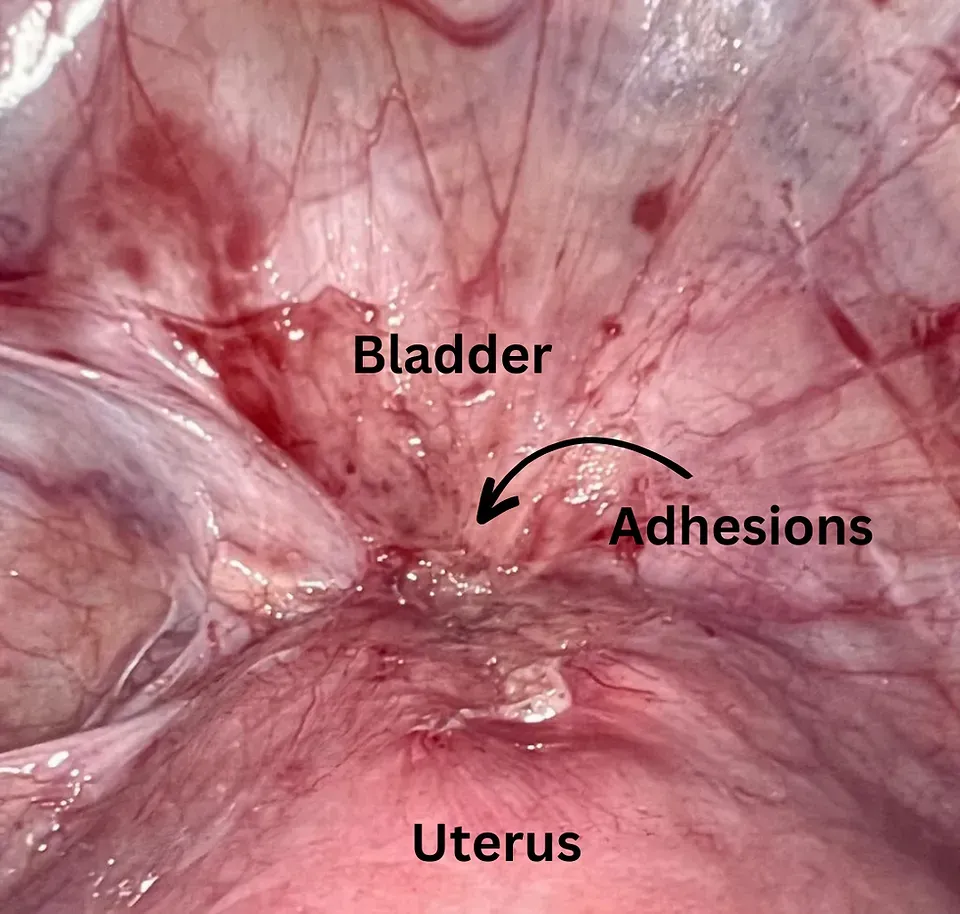
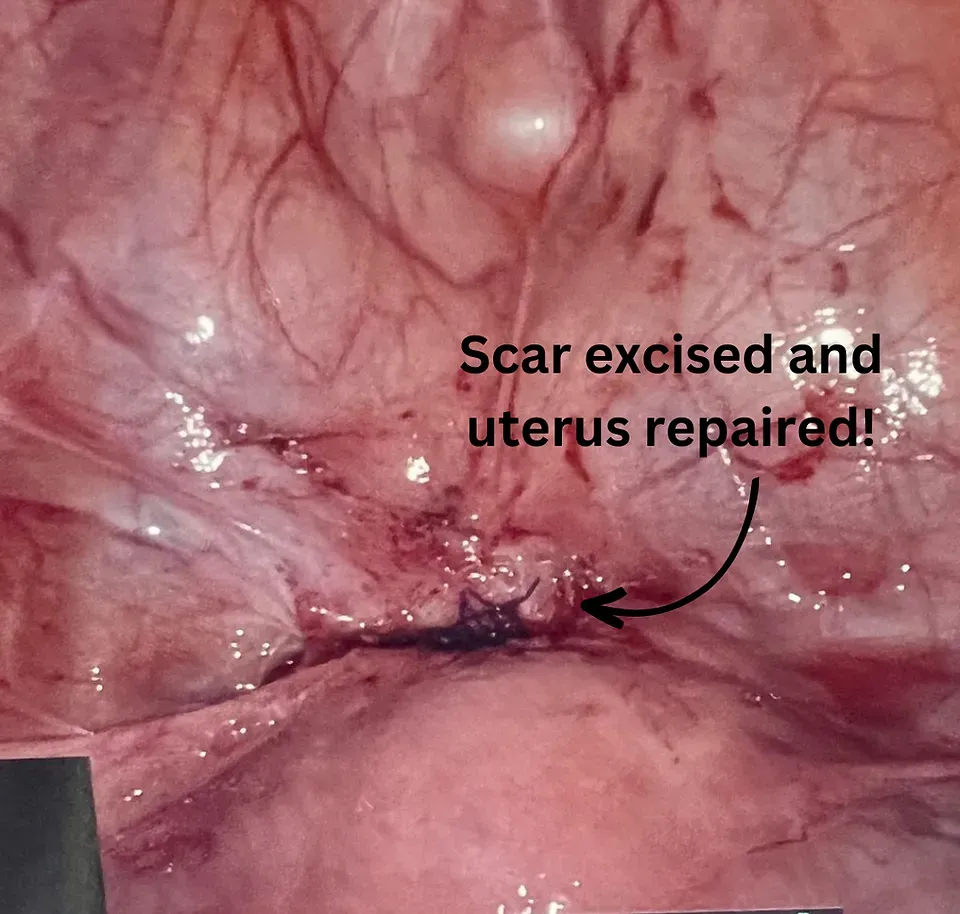
Cesarean Scar-Defect Repair
Did you know that almost one third of babies in the United States are born by c-section? While c-sections can be wonderful aids to a healthy-mom-healthy-baby delivery, they can pose some issues postpartum if someone develops a cesarean scar defect.
More Surgical Treatments
- Robotic surgery
- Advanced hysteroscopy
- Myomectomy (fibroid removal)
- Excision of endometriosis
- Robotic, laparoscopic, and vaginal hysterectomy
- Ovarian cyst removal
- Ovarian wedge resection
- Tubal reversal
- Tubal recanalization
- Cesarean scar defect (isthmocele) removal
- Robotic transabdominal cerclage
- Vaginal cerclage
- Labioplasty
- Vaginal surgery
- Pelvic floor trigger point injections
- Pelvic floor Botox injections
- Endometrial ablation
- Uterine / cervical polypectomy
- Lysis of uterine adhesions
- Lysis of pelvic adhesions
